The student knows the symptoms of life-threatening hypo-/hyperkalaemia The student knows the relationship between acid-base imbalance and the value of hypo-/hyperkalemia The student knows the typical ECG changes in hypo-/hyperkalemia
The student knows the indications to perform acute elimination in intensive care (hypervolemia, acidemia, hyperkalemia, uremia, ev. toxin)
Below is a summary of the chapter content. The topic is described in detail in the Oxford Handbook of Critical Care (see below).
Hyperkalemia
Hyperkalemia serum K+ level > 5.5 mmol/l. Severe hyperkalaemia with K+ > 6.5 mmol/l with ECG changes.
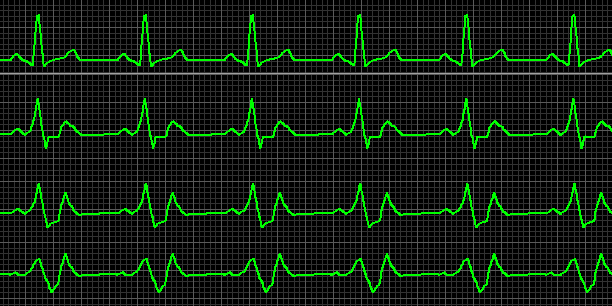
1st line sinus rhythm in other lines, changes with the progression of hyperkalemia: (K+ 6-7 mmol/l: high spiked T, QT shortening) (K+ 7-8 mmol/l: QRS widening, disappearance of P waves) (K+ > 8mmol/l: bizarre wide QRS) risk of ventricular fibrillation and asystole increases with increasing K+ levels
Treatment of hyperkalaemia according to European Resuscitation Council Recommendation 2021
In circulatory arrest with hyperkalaemia
in addition to the above-mentioned medication, 50 ml of 8.4% sodium bicarbonate IV is indicated.
Hypokalemia
Hypokalemia serum K+ level < 3.5 mmol/l. Severe hypokalaemia with K+ < 3 mmol/l.
In critical patients with hypokalemia, intravenous replacement is appropriate; oral administration is slow, and absorption is unpredictable.
When administered by peripheral cannula, the maximum rate of potassium administration may be 10 mmol/h at a maximum concentration of 40 mmol/l.
This corresponds to 35ml of 7.45% KCl added to 1000ml of most balanced solutions (where the usual potassium concentration is 4-5mmol/l) with a maximum infusion rate of 250ml/hr.
Higher concentrations and rates of KCl administration can only be administered via a central venous catheter (CVC), and the patient must be connected to continuous ECG monitoring. In practice, concentrated KCl solutions of 7.45% (1mmol/l) are used up to a maximum rate of 20mmol/hr with frequent ionogram checks.
When substitution is used, it is advisable to check the ionogram, especially Mg levels and substitute it if necessary.
The relation to blood pH and the level of kalemia should always be considered.
Caution should be taken with 'normal reference levels' of kalaemia in patients with severe acidosis (e.g. diabetic ketoacidosis), often requiring significant replacement.
Indications for RRT (Renal Replacement Therapy)
The topic of elimination methods itself is complex and specialized. We consider it to be the domain of the Intensive Care or Nephrology Departments and beyond the scope of this chapter and the required knowledge of students in the Intensive Care Medicine course. However, the indication to consider initiating elimination methods is essential knowledge for any physician, allowing just a consultation with an intensivist or nephrologist.
The indication for RRT should always be considered individually, considering the trend of the patient's condition, the response to other therapeutic steps and goals.
Hyperkalaemia (K+ >6.5mmol/l), which is unresponsive to conservative therapy, and other ionic imbalances (hyperMg, hyperCa, disorders of natremia) are not so common. Always consult a specialist.
Refractory metabolic acidosis (MAc) with kidney injury
Severe hyperkalemia is often the result of metabolic acidosis (MAc), a shift from the intracellular space. Severe MAc (pH < 7.1) also indicates the initiation of RRT.
The relationship between pH and K+ levels is discussed in more detail in the chapter Acid-Base Disorders.
Fluid overload without adequate response to diuretic administration (in oligo-/anuria) (in the presence of other organ dysfunctions, an early indication of RRT before actual congestion is also to be considered)
Nitrogen retention, uremic syndrome Usually urea >30-40 mmol/l, some sources include creatinine >300 μmol/l as an indication (in critical patients, values alone are not as important in the indication as in chronic patients)
Intoxication (lithium, metformin, toxic alcohols,...) Toxnet or Nephrologist can be consulted if the toxin can be eliminated by RRT methods (see chapter Intoxication)
Initiation of RTT requires a special intravenous cannula, which must be secured before starting the method. It is advisable to contact the consultant early.
RRT is an invasive method with possible serious systemic complications.
Ultrasound examination of the kidneys and urinary tract should be performed to rule out postrenal causes of renal failure before starting RRT.
Recommended reading for this chapter:
Oxford Handbook of Critical Care. SINGER Mervyn, WEBB R. Andrew