Posture and functional musculoskeletal disorders
Postural functions
Postural function is a dynamic process, which ensures active muscle hold of individual body segments against external, gravitational force (during physical performance the external force also includes e.g. inertia friction force, reaction force, the resistive force of the athlete).
Postural functions:
- ensures that the upright (bipedal) labile body position is kept and maintained during changing conditions in the gravitational field,
- is a phylogenetic precondition for every human movement,
- is the result of complex reflex processes that are programmed in the CNS (proceeding according to precise pre-determined rules),
- is a multifactorial process running throughout the life, evolving from birth and requiring increased attention at all stages of ontogenesis,
- it’s quality is very unstable, has considerable compensatory and substitution options,
- is genetically determined (internal influences),
- is positively and negatively influenced by the lifestyle (external influences),
- three reciprocally linked components, a sensory, controlling and executive component, working as a single functional unit, are involved in its implementation.
The quality of the postural function, i.e. the physiological posture (correct posture - "CP") is an indirect indicator of health.
It is important not only in terms of functionality of support and targeted motor skills, but it also affects the activity of other body systems (respiratory, cardiovascular, digestive, excretory ... - vertebrovisceral relationships).
The psychological condition also affects the quality of the posture (mental fatigue, stress = a stress-limiting reaction to the organism, so-called somatization of psychic tension).
Factors characterizing the quality of posture:
- static component - physiological shape of the spine (pelvic slope, chest shape, the position of the lower limbs, and the ach of the foot),
- dynamic component - optimal resting tone of postural muscles, physiological interplay of antagonistic and synergistic muscle groups (muscular balance), physiological movement stereotypes,
- optimal functional status of the organism (nervous system - mental level, hypothalamic - pituitary system, transport system),
- psychological characteristics (self-confidence, the current mood, social status in a group),
- the quality of posture also affects body structure (somatotype), fatigue, nutrition, drinking regime, clothing, footwear ...
In every movement, it is possible from didactic reasons to distinguish:
- the "holding" component (moving, supporting),
- the "movement" component (kinetic, locomotive).
Both systems convey two sides of the same process:
- are equal,
- reciprocally related,
- they cannot be separated from each other.
In the physical education process, equal attention must be paid to both systems and not to place a "motion" component above all (often we are only interested in the performance itself). This way the stimulating organism can successfully resist negative effects of the current lifestyle, minimize damage to the motor system and to help optimize the level of motor skills and training of movement skills. The static and consequent dynamic stability of the body in motion involves a deep stabilization system of the spine, to which the activity of superficial muscles should be linked according to the intensity of the movement (stand versus stand without visual control (e.g. on bosu, balance platform).
Regular placement of intentional interventional motion programs positively influencing the quality of postural function is essential.
Correct Posture
The posture is a complex concept that represents a certain standard called - Ideal standing, in which the segments of the main body segments are directly linked (each segment is above the lower one) so the sum of the forces that disturb the balance in the individual bone connections is minimal (Kopřivová & Kopřiva, 1997).
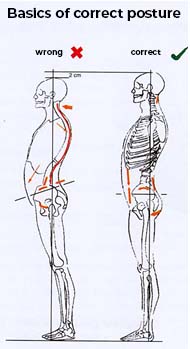
The correct posture is important not only from an aesthetic point of view but especially for health reasons. With proper body posture, inappropriate loading can be prevented, which means that not only joints are protected, but also organs have enough space. Muchová & Tománková (2009) point out that, in a fictitious correct posture, the legs are naturally stretched freely with each other, knees and hips are naturally stretched. The pelvis is in such a position that the body weight is above the line connecting the centers of the hip joints. The spine is continuously curved. The shoulders are lowered downwards and are slightly attached to the spine. The head is upright, the chin is in a right angle with the body axis. Figure 1 shows the difference especially seen in lumbar lordosis and thoracic kyphosis in the correct and incorrect posture.
Inorrect posture causes muscle tension and reduced mobility, which can cause injuries (Bimbi – Dresp, 2007).
The Assessment of posture is usually done in a standing position. According to Hálková (2001) the ideal position looks like that seen in Figure 1:
The principles of proper sitting
In upright sitting (Figure 2), the pelvis should be tipped slightly forward, and the spinal curvature of the spine should be maintained. In the case of long-term stresses, such as the back or head inclination, the asymmetric pressure may damage the discs. The chest should remain open, use the abdomen to breathe in and the shoulders should be loose. Also important is the position of the legs, which should be straddled, the angle between the thighs should not be less than 45° and the hips remain slightly above the knees. Due to the fact that not all activities can be performed in the upright sitting position, it is possible to choose so-called inclined sitting (Figure 3), which looks like we lean over the table with a straight spine. In this case, there is a greater bend in the hip and inclination of the pelvis. The elbows should rest against the table top and the elbow joints are at a 90° (Muchová & Tománková, 2010).
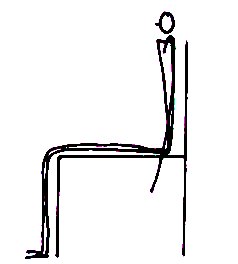
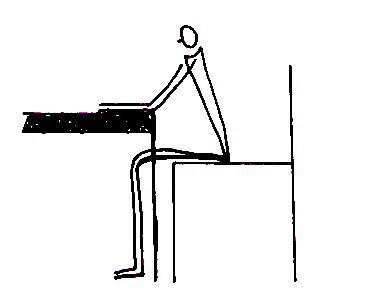
Fig.3. inclined sitting
Anatomy of Spine
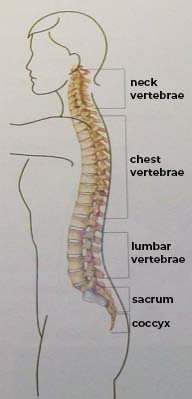
The spine (Figure 4) forms the longitudinal axis of the skeleton, carries the head, supports the torso and consists of a total of 24 vertebrae:
- seven in neck,
- twelve in chest
- five in the lumbar section, which is followed by the sacrum and coccyx.
Two vertebral arches are routed from each vertebra, pointing backwards, joining together to form a vertebral opening. The spinal cord passes through the canal, which is formed by the vertebrae. The intervertebral discs are located between the vertebrae and act as shock absorbers. A healthy spine is in the form of a double S shaped, in such a way that the cervical and lumbar vertebrae are slightly bent forward, and the thoracic vertebrae are slightly bent backward (Bimbi – Dresp, 2007).
The functional ability of the spine is affected not only by the condition of vertebrae, joints, disks and ligaments but also the condition of the muscles, therefore it should be stressed that functional stability of the spine is provided by a muscle corset.
The most important muscles around the spine include rotators and erector spinae. Rotators are short muscles that are located diagonally between the vertebrae and belongs to the muscles which tend to weaken. Erector muscles of the torso have the tendency to shorten and they are the muscles that lie longitudinally around the spine (Tlapák, 1999).
Spinal health problems which may occur, include:
Hypokyphosis
Hypokyphosis (Figure 5) also called round back is discussed, as having an increased curvature of the thoracic spine. This is the acquired postural defect, which often occurs in children who have different health problems (Kopřivová, Kopřiva, 1997). hypokyphosis is the result of muscle imbalances, shortened pectoral muscles, and weakened inter blade muscles and lower portions of the trapezius muscle (Syslová, 2005).

Scoliosis
Another spinal disorder that we may encounter is scoliosis (Figure 6). We talk about it when we meet the secondary curvature of the spine, to the side which is often associated with rotation of the spine. Scoliosis may be genetically inherited however, if this is not a genetic matter, it can be caused by repeated activity, such as carrying a heavy shoulder bag. In case of severe scoliosis, the position of the ribs may be affected which can interfere with the natural placement of internal organs. As a result, from these problems, neurological problems may arise which created pressure on the nerves and finally can exhibit problems with the lungs. The secondary curvature, appearing in the lower part of the spine, may also affect the upper spine if one tries to compensate for the lower back (Blount & McKenzie, 2005).

Hypolordosis
Hypolordosis (Figure 7) can be characterized as excessive bending in the area of the lumbar spine which results in the abdomen being pulled forward (Blount & McKenzie, 2005). It occurs due to the shortened spinal extensors of the spine in the lumbar region, also due to the weakening of rectus abdominis (Syslová, 2005).

Flat back
Hypolordosis (Figure 7) can be characterized as excessive bending in the area of the lumbar spine which results in the abdomen being pulled forward (Blount & McKenzie, 2005). It occurs due to the shortened spinal extensors of the spine in the lumbar region, also due to the weakening of rectus abdominis (Syslová, 2005).

In general, we can say that these disorders develop gradually, which can be removed with proper exercise, when the functional malfunctions first occur; however, if this correction does not occur, structural changes will appear and the defect, the defect is unfortunately impossible to be removed (Kopřivová & Kopřiva, 1997).
Functional disorders of the locomotive apparatus
Functional disorders of the locomotor system are disorders of the joints, muscles, nerves, other soft tissues, organs, organ systems and the whole organism, when the organic, structural cause is not the primary reason for the disease. Functional malfunction is then a malfunction of the control function.
Functional disorders of the locomotor apparatus are most clearly manifested in three system interconnected levels (Kolář, 1997):
- in the area of muscle function – muscle imbalance;
- in the area of central regulation – disturbances of movement stereotypes;
- in the area of joint function – restriction of joint mobility or hypermobility.
Muscle function is greatly influenced by the movement mode. Hypokinesis, unilateral stress and mental tension are the most frequently cited causes of undesirable functional changes in the muscular system. As a result of unilateral load, the excessively strong and short muscles and over-weakened muscle groups are created. It has been shown that these changes have a deeper physiological basis, which is based on the distinction of the muscles. Neuromuscular complex remains the leading cause of functional disorders which are not paresis, but the inhibition of muscle activity. We cannot speak purely about muscle disorders because the muscle and the nerve cannot be separated from each other. The muscle is taken as the output of the nervous system or disorders afferent to which the management is directly dependent. Musculoskeletal disorders are often the cause of pain and its prolonged duration cause prominent morphological changes inducing central changes, which can be identified and effectively influenced. It is essential that function failure occurs as a cause and a consequence of morphological disorders of the locomotive apparatus. Each disorder of the postural function is manifested by a pathological change of some parts of the locomotive apparatus but is not associated with a change in its structure.
Shortening and weakening of the muscle
Muscle shortening is a condition where the muscle does not reach its normal physiological length, and in passive movement in the joint, it will not allow the abrupt muscle to reach the full physiological range of motion in the joint that transcends and can still flex the joint from the zero position. We distinguish two degrees of shortening:
- slight shortening
- significant shortening
If the muscle is only slightly shortened under the load, this muscle is stronger and at the joint there is an advantage transfer of the muscular force from the initial position which may be an advantage in certain cases (e.g. in elite athletes). With a significant shortening, the muscle loses its elasticity and, after a certain amount of time, also its strength. From a functional point of view, the shortened muscle can not only lead to a change in the movement stereotype but also to change static ratios mainly during walking and working activities. The muscle is activated in situations where it should not be activated. In activities it is more involved in the function, which leads to the overloading of the locomotive apparatus. At the same time, it acts as a buffer to its antagonists, so the weakened, predominantly phasic muscles cannot be fully strengthened without first stretching the predominantly postural muscles.
There are two types of muscle groups:
1. Postural muscles - muscles with a tendency to shorten
- neck muscles,
- the upper part of the trapezius muscle and levator scapulae muscle,
- pectoralis major and minor muscles,
- lumbar muscles (lumbar part of erector spinae, quadratus lumborum),
- hip flexors (iliopsoas muscle and rectus femoris muscle),
- adductors muscles,
- knee flexors,
- gastrocnemius and soleus.
The main principles of proper stretching of the postural muscles:
- include relaxation exercises before stretching,
- approach exercise completely relaxed and under the condition of moderate warm up,
- choose the most stable and comfortable positions to stretch,
- focus attention on the muscle being stretched,
- move smoothly and slowly,
- no pain should occur during stretching,
- we choose the optimum stretch time (10 to 20 seconds),
- calmly and regularly breathe when stretching,
- the effect of stretching will last only a day, and if the shortened muscle does not get stretched within 48 hours, it will be shortened again.
Stretching techniques
- passive static stretching,
- post isometric relaxation (tension - relaxation – stretching),
- dynamic stretching through swift, swinging movements.
2. Phasic muscles - muscles with a tendency to weaken
- head and neck flexors,
- mid-scapular muscles (rhomboids and middle part of the trapezius muscle),
- lower part of the trapezius,
- abdominal muscles,
- gluteus maximus, medius and minimus,
- some parts of the knee extensors (quadriceps),
- the muscles on the front and side of the lower leg.
The main principles of proper strengthening of phasic muscles:
- stretch its shorten antagonist,
- learn to activate the weak muscle and gradually engage it in the correct movement stereotype,
- after mastering the technique of motion gradually increase the number of repetitions (up to 10-15),
- first strengthen without additional load (against the gravity),
- then increase the difficulty and complexity of the exercise through different body positions,
- only after perfect adaptation approach the use of external resistances,
- coordination with the breath is very important.
Muscular disbalance
Muscle imbalance develops from inappropriate, unilateral loading of the locomotor system without subsequent compensation, lack of exercise and overloading when the differences between the muscle groups greatly accentuate. The static nature of the load straining the postural muscles which then are considerably shortened. Lack of versatile physical activity causes a reduction in muscular muscle strength with predominantly phasic functions. When the balance is maintained between the agonistic and antagonistic muscles, the muscles are able to work together to control a certain area of the body. In other words, under normal circumstances, the muscle tension on the opposite sides of the joints is balanced, in order to ensure the proper and therefore correct holding of the relevant body segment. If there is a relatively greater activation of the muscles with predominantly static function, these muscles tend to dominate and creating shorten muscle groups. The original physiological balance between the two systems is thus disturbed in the sense of predominance of the system with predominantly postural function. This results in muscle imbalance or disbalance. This has a negative effect on muscle tone and can lead to structural changes. Shorten muscle based on reflexive and development of relations has a dampening effect on the weaken phasic muscle. The function of weaken muscles takes over the muscles shorten, thereby further deepens the imbalance (Janda. 1982).
We can distinguish between two types of muscular disbalance (by Tlapák, 2004):
- Local – in a certain muscle unit.
- Systemic – throughout the musculoskeletal system which results from the unbalance of the dynamic one-sided load and thus the overload of the locomotive apparatus. Muscles engage in motion differently than when they are performing economical movements, and there is a disruption of muscle coordination.
Typically, we find muscular disbalance associated with syndromes. Following are the main syndromes:
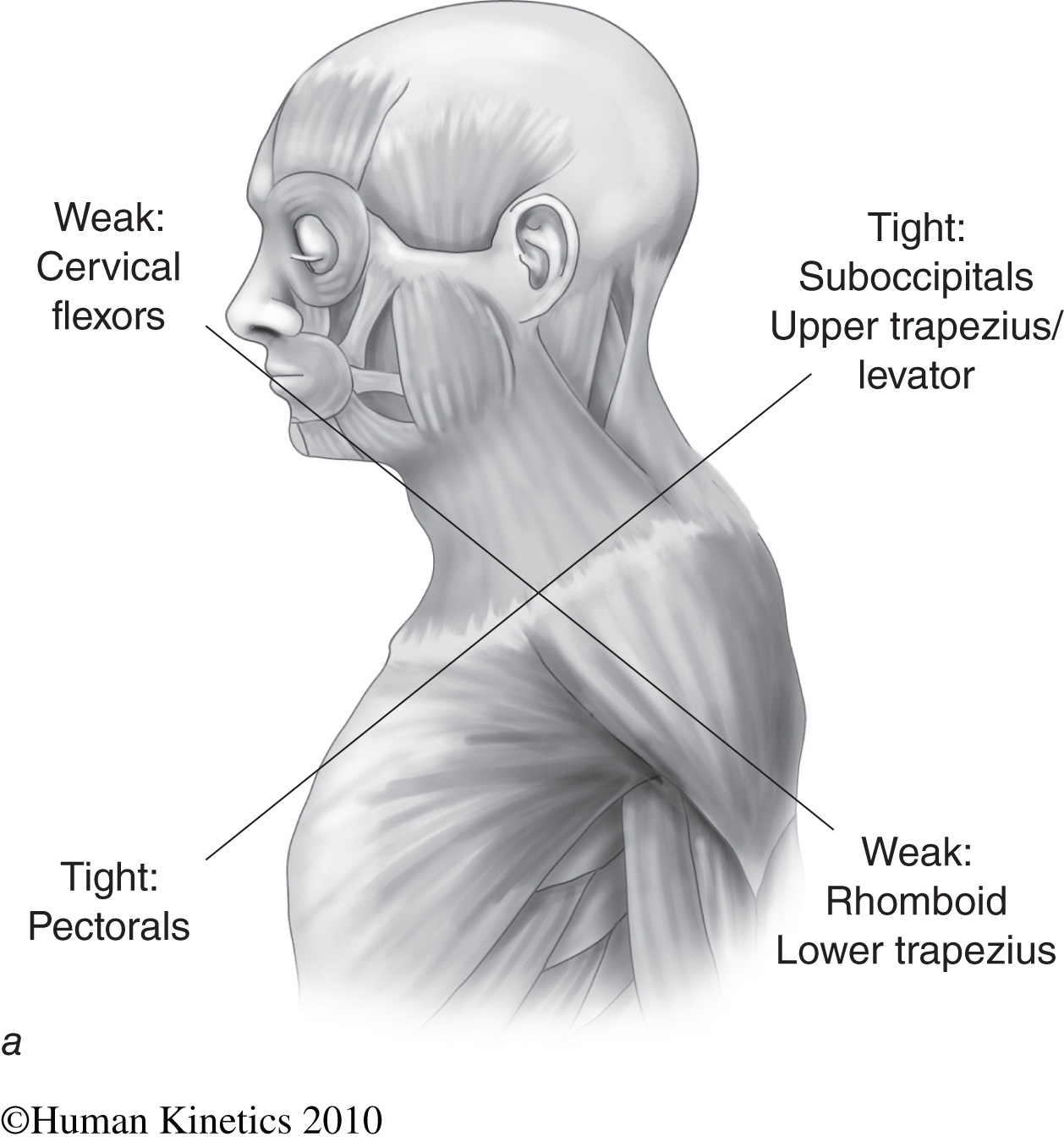
1. Upper cross syndrome
In this syndrome, there is a shortening of the upper trapezius muscle fibers and levator scapula and the predominance the neck flexors. One of the most commonly shorten muscles are pectoralis major and minor. Deep neck flexors and lower blade fixators are weakened. Also, the muscles along the spine in the chest segments tend to be relatively weaker. The below mentioned muscular disbalance (Figure 9) is accompanied by a significant change in the statics and dynamics of the motor stereotypes. The head shifts forward with overload of the cervical and thoracic transition, cervical hypolordosis is promoted by shortening the trapezius (the upper part). The so-called Gothic shoulders are formed with the elevation of the entire shoulder girdle round the back and bottom of the projection angle or the inner edge of the blade lifts from the chest. This imbalance leads not only to a static overload of the cervical and thoracic segments of the spine, but it is also a prerequisite for changes in the motor stereotypes in the area of the shoulder girdle. These are manifested practically in all movements in the shoulder joint.
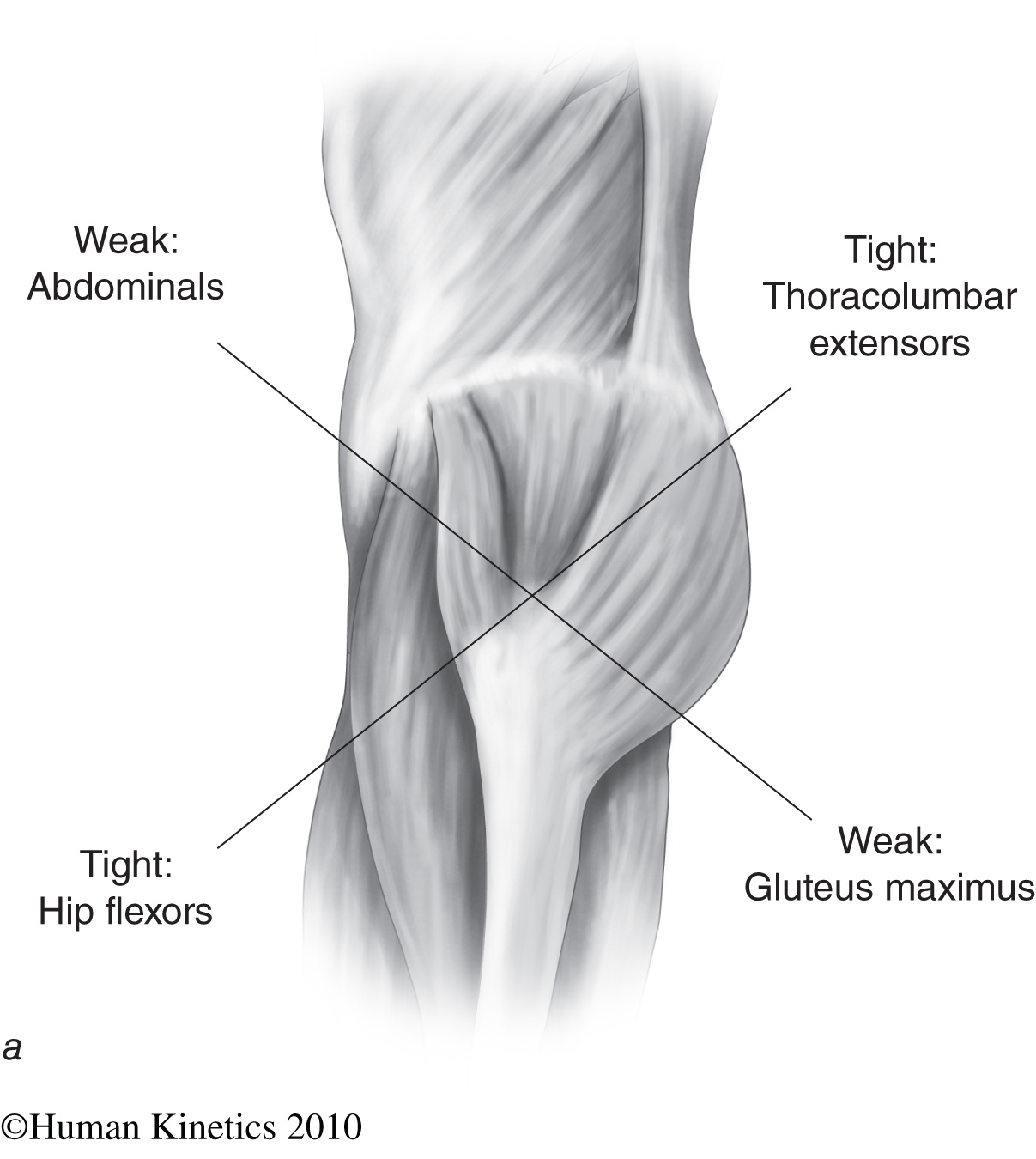
2. Lower crossed syndrome
In this syndrome (Fig. 10) there are shortened hip flexors (iliopsoas, rectus femoris, fascia lata), erector spinae muscle group, those in the transition of lumbar and sacral areas, not thoracic. There is attenuation and weakening of the gluteus muscles, maximus, medius and minimus. Strengthening of the gluteus muscles is important and is essential for body posture. Abdominal muscles are weakened. Weakening of the abdominal muscles is considered one of the most common causes of lumbar hypolordosis. However, the imbalance of all four of these groups is required to produce hypolordosis. This imbalance leads to a change in static and dynamic ratios. The pelvis is tilted forward, the hip joint is in flexed position and there is an increased lordosis in the lumbar and sacral transition region. It is accompanied by a change in distribution of pressure on the hip joints and on the cross and lumbar segments.
The consequences of muscular disbalance may have both local and general character and it can become a source of pathogenic stimuli for further deepening of muscle imbalance. This can lead to distortions of static and dynamic function of the musculoskeletal system, as well as to the defects in the programming of the body posture and mobility within the central nervous system. It is also important to emphasize that muscle imbalances are the precursor or the first stage of very severe functional disorders of the locomotor system. Due to impaired muscular balance we can deduce the predominant part of postural defects, that is, poor posture in children and youth, and in it we can see one of the main causes of functional failure in the vertebral spine difficulties in adulthood (Čermák, Chválová & Botlíková, 1998).
These functional disorders can be mitigated or removed by proper exercise, it is one of the bodystyling goals. Also important is proper exercise technique and selection of appropriate exercises.